Pharmacotherapeutic group: Psycholeptics, other antipsychotics.
ATC code: N05AX12.
Pharmacology: Pharmacodynamics: Mechanism of action: The mechanism of action of aripiprazole, as with other drugs having efficacy in schizophrenia or bipolar I disorder is unknown. However, it has been proposed that aripiprazole's efficacy in schizophrenia is mediated through a combination of partial agonism at dopamine D2 and serotonin 5-HT1A receptors and antagonism at serotonin 5-HT2A receptors. Aripiprazole exhibited antagonist properties in animal models of dopaminergic hyperactivity and agonist properties of dopaminergic hypoactivity. Aripiprazole exhibits high binding affinity
in vitro for dopamine D2 and D3, serotonin 5-HT1A and 5-HT2A receptors and has moderate affinity for dopamine D4, serotonin 5-HT2C and 5-HT7, alpha-1 adrenergic, and histamine H1 receptors. Aripiprazole also exhibited moderate binding affinity for the serotonin reuptake site and no appreciable affinity for cholinergic muscarinic receptors. Interaction with receptors other than dopamine and serotonin subtypes may explain some of the other clinical effects of aripiprazole.
Aripiprazole oral doses ranging from 0.5 to 30 mg administered once a day to healthy subjects for 2 weeks produced a dose-dependent reduction in the binding of
11C-raclopride, a D2/D3 receptor ligand, to the caudate and putamen detected by positron emission tomography.
Further information on clinical trials: Clinical Efficacy in Maintenance treatment of schizophrenia in adults: The efficacy of Abilify Maintena in the maintenance treatment of patients with schizophrenia was established in two randomised, double-blind trials.
The first trial was a 38 week, randomised, double-blind, active-controlled trial designed to establish the efficacy, safety, and tolerability of this medicinal product administered as monthly injections compared to once daily oral aripiprazole tablets 10-30 mg as maintenance treatment in adult patients with schizophrenia. This trial consisted of a screening phase and 3 treatment phases: Conversion Phase, Oral Stabilisation Phase, and Double-Blind, Active-Controlled Phase.
Six-hundred and sixty two patients eligible for the 38-week Double-Blind, Active-Controlled Phase were randomly assigned in a 2:2:1 ratio to double-blind treatment to one of 3 treatment groups: 1) Abilify Maintena; 2) the stabilisation dose of oral aripiprazole 10-30 mg, or; 3) aripiprazole Long-Acting Injectable 50 mg/25 mg. The aripiprazole Long-Acting Injectable 50 mg/25 mg dose was included as a low dose aripiprazole group to test assay sensitivity for the non-inferiority design.
The results of analysis of the primary efficacy endpoint, the estimated proportion of patients experiencing impending relapse by end of Week 26 of the Double-blind, Active-controlled Phase, showed that Abilify Maintena 400 mg/300 mg is non-inferior to aripiprazole oral tablets 10-30 mg.
The estimated relapse rate by end of Week 26 was 7.12 % in the Abilify Maintena group, and 7.76 % in the oral aripiprazole tablets 10-30 mg group, a difference of -0.64 %.
The 95 % CI (-5.26, 3.99) for the difference in the estimated proportion of patients experiencing impending relapse by end of Week 26 excluded the predefined non-inferiority margin, 11.5 %. Therefore, Abilify Maintena is non-inferior to the aripiprazole oral tablets 10-30 mg formulation.
The estimated proportion of patients experiencing impending relapse by end of Week 26 for the Abilify Maintena group was 7.12 %, which was statistically significantly lower than in the aripiprazole Long-Acting Injectable 50 mg/25 mg group (21.80 %; p = 0.0006). Thus, superiority of Abilify Maintena over the aripiprazole Long-Acting Injectable 50 mg/25 mg was established and the validity of the trial design was confirmed.
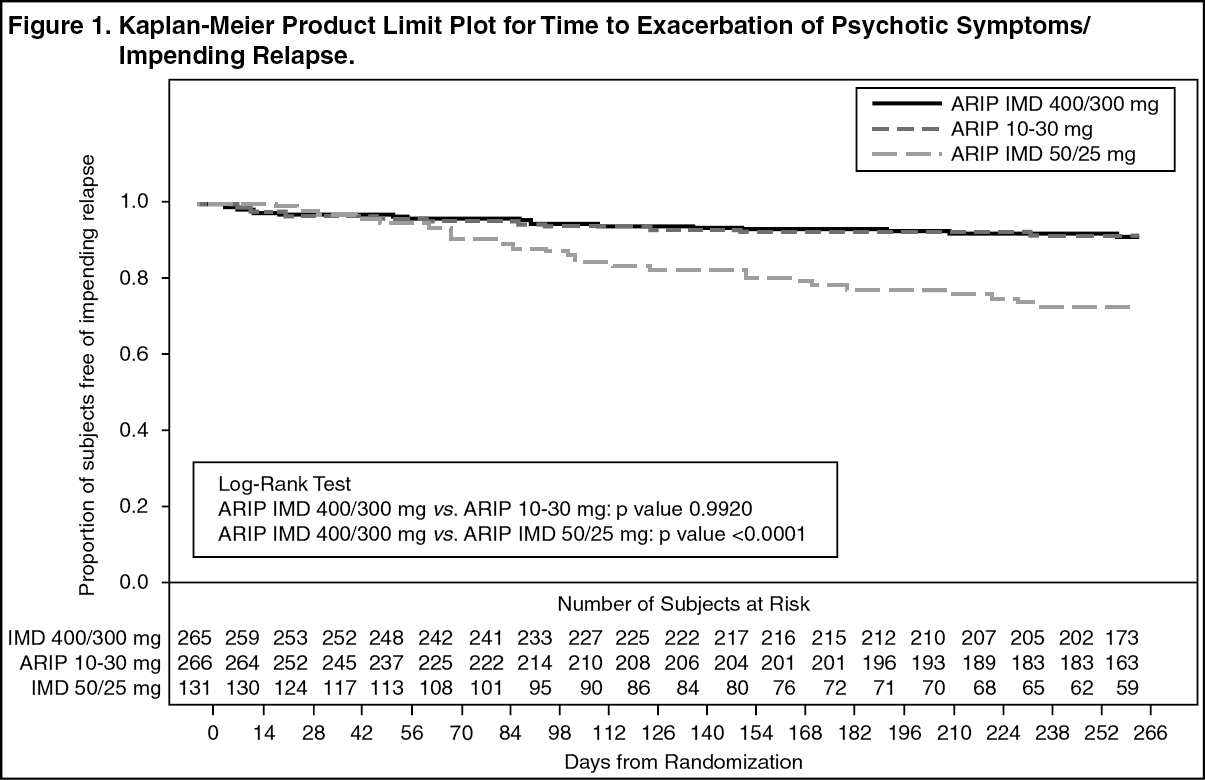
The Kaplan-Meier curves of the time from randomisation to impending relapse during the 38-week, double-blind treatment phase for Abilify Maintena, oral aripiprazole 10-30 mg group, and aripiprazole Long-Acting Injectable 50 mg/25 mg groups are shown in Figure 1. (See Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
NOTE: ARIP IMD 400/300 mg = Abilify Maintena; ARIP 10-30 mg = oral aripiprazole; ARIP IMD 50/25 mg = Long-acting Injectable.
Further, the non-inferiority of Abilify Maintena compared to oral aripiprazole 10-30 mg is supported by the results of the analysis of Positive and Negative Syndrome Scale for Schizophrenia (PANSS). (See Table 1.)
Click on icon to see table/diagram/image
The second trial was a 52-week, randomised, withdrawal, double-blind, trial conducted in adult patients with a current diagnosis of schizophrenia. This trial consisted of a screening phase and 4 treatment phases: Conversion, Oral Stabilisation, Abilify Maintena Stabilisation, and Double-blind Placebo-controlled. Patients fulfilling the oral stabilisation requirement in the Oral Stabilisation Phase were assigned to receive, in a single-blind fashion, Abilify Maintena and began an Abilify Maintena Stabilisation Phase for a minimum of 12 weeks and a maximum of 36 weeks. Patients eligible for the Double-blind, Placebo-controlled Phase were randomly assigned in a 2:1 ratio to double-blind treatment with Abilify Maintena or placebo, respectively.
The final efficacy analysis included 403 randomised patients and 80 exacerbations of psychotic symptoms/impending relapse events.
The study was terminated early because efficacy was demonstrated by the pre-specified interim analysis. The hazard ratio from the Cox proportional hazard model for the placebo to Abilify Maintena comparison was 5.029 (95 % CI = 3.154, 8.018); thus patients in the placebo group had a 5.03-fold greater risk of experiencing impending relapse than patients in the Abilify Maintena group. This results support efficacy for Abilify Maintena over 52 weeks of treatment.
The Kaplan-Meier curves of the time from randomisation to impending relapse during the 52-week, double-blind treatment phase for Abilify Maintena and placebo groups are shown in Figure 2. (See Figure 2.)
Click on icon to see table/diagram/image
The percentage of patients meeting the impending relapse criteria was significantly lower (p < 0.0001) in the Abilify Maintena group (10.0 %) than in the placebo group (39.6 %).
Further, the superiority of Abilify Maintena compared to placebo is supported by the results of the analysis of PANSS. (See Table 2.)
Click on icon to see table/diagram/image
Clinical Efficacy in the Acute Phase of Schizophrenia: The efficacy of Abilify Maintena in adult patients in the acute phase of schizophrenia was established in one short-term (12-week), randomized, double-blind, placebo controlled trial of acutely relapsed adult patients. In this trial, the primary measure used for assessing psychiatric signs and symptoms was the Positive and Negative Syndrome Scale (PANSS). The primary endpoint was the change from baseline to week 10 in PANSS total score. The key secondary endpoint was the Clinical Global Impression-Severity (CGI-S) assessment at week 10.
The inclusion criteria for this short term trial included adult inpatients who met DSM-IV-TR criteria for schizophrenia. In addition, all patients entering the trial must have experienced an acute psychotic episode as defined by both PANSS Total Score ≥ 80 and a PANSS score of > 4 on each of four specific psychotic symptoms (conceptual disorganization, hallucinatory behavior, suspiciousness/persecution, unusual thought content) at screening and baseline. Patients had a mean PANSS total score of 103 (range 82 to 144) and a CGIS score of 5.0 (markedly ill) at entry.
In this 12-week study (n=339) comparing Abilify Maintena (n=167) to placebo (n=172), patients were administered 400 mg Abilify Maintena or placebo on days 0, 28, and 56. The dose could be adjusted down and up within the range of 400 to 300 mg on a one time basis. (For the first two weeks of the study, subjects randomized to Abilify Maintena also received concomitant oral Abilify Maintena, 10 to 20 mg/day). Abilify Maintena was superior to placebo in improving the PANSS total score with early onset and sustained efficacy (week 10 scores of -26.8 vs. -11.7 respectively) with a statistical difference at each measured time point, p=<0.0005 at week 1 and p=<0.0001 for all other time points until study completion. The adjusted mean change in PANSS total score over time (Mixed Model of Repeated Measure MMRM) is demonstrated in Figure 3. (See Figure 3.)
Click on icon to see table/diagram/image
Abilify Maintena also showed improvement in CGI-S score mean changes from baseline that were statistically significant at all post-baseline timepoints (week 10 scores of -1.4 vs. -0.6 at week 10, Abilify Maintena vs. placebo, respectively).
Clinical Efficacy in Maintenance Treatment of Bipolar I Disorder: The safety and efficacy of Abilify Maintena as maintenance treatment in adults with bipolar I disorder aged 18 to 65 years was demonstrated in a 52-week multicenter, randomized, double-blind, placebo-controlled trial (Trial 31-08-250) of patients who met DSM-IV-TR criteria for bipolar I disorder and who were currently experiencing a manic episode at trial entry.
This trial consisted of a screening phase and 4 treatment phases: An oral conversion phase (4 to 6 weeks) for all subjects to achieve a monotherapy target starting dose of 15 mg/day oral aripiprazole. A total of 466 patients entered this phase.
An oral stabilization phase (a minimum of 2 weeks and a maximum of 8 weeks in duration) during which subjects were stabilized on an oral dose of aripiprazole ranging from 15 mg to 30 mg daily. Stabilization was defined as having all of the following stability criteria at one biweekly visit in order to proceed to Abilify Maintena stabilization phase: outpatient status, YMRS total score ≤ 12, MADRS total score ≤ 12, no active suicidality; with active suicidality defined as a score of 4 or more on the MADRS item 10 OR an answer of "yes" on question 4 or 5 on the Columbia Suicide Severity Rating Scale (C-SSRS). A total of 632 patients entered this phase of which 265 patients entered the oral stabilization phase directly.
Abilify Maintena Stabilization Phase (a minimum of 12 weeks and a maximum of 28 weeks in duration) during which subjects were stabilized on Abilify Maintena 400 mg or 300 mg, as dictated by tolerability. Oral dosing with aripiprazole continued for the first 2 weeks following the injection to maintain therapeutic plasma concentrations. Stabilization was defined as having all of the following for eight consecutive weeks: an outpatient status, YMRS total score ≤ 12, MADRS total score ≤ 12, no active suicidality; with active suicidality defined as a score of 4 or more on the MADRS item 10 OR an answer of "yes" on question 4 or 5 on the Columbia Suicide Severity Rating Scale (C-SSRS). A total of 425 patients entered this phase. The mean baseline YMRS total score was 5.8 (range, 0 to 28). The mean baseline MADRS total score were 3.7 (range, 0 to 28). The mean baseline CGI-BP-S overall score was 2.1 (range, 1 to 5). Patients who demonstrated stability for 8 consecutive weeks were randomized into the double-blind, placebo-controlled treatment phase.
A randomized, double-blind, placebo-controlled phase (52 weeks). Two hundred sixty six (266) patients eligible for the 52-week double-blind, placebo-controlled phase were randomly assigned in a 1:1 ratio to double-blind treatment with either the last stabilization dose of Abilify Maintena from the previous phase or placebo. During this phase, a single decrease to Abilify Maintena 300 mg was permitted for tolerability, as was a single return to the original 400 mg dose if required. The mean baseline YMRS total score was 2.9, and 2.6 for the Abilify Maintena 400 mg/300 mg and placebo groups, respectively. The mean baseline MADRS total score was 3.0 and 2.4 for the Abilify Maintena 400 mg/300 mg and placebo groups, respectively. The mean baseline CGI-BP-S score was 1.5 and 1.4 for the Abilify Maintena 400 mg/300 mg and placebo groups, respectively.
The primary efficacy endpoint of this trial was the time from randomization to recurrence of any mood episode during the double-blind, placebo-controlled phase.
The time to recurrence of any mood episode was significantly longer in subjects randomized to the Abilify Maintena group compared to placebo-treated subjects. A total of 103 mood events were observed during the double-blind treatment phase: 35 occurred during Abilify Maintena treatment and 68 occurred during placebo treatment (26.5% vs 51.1%, p < 0.0001). The hazard ratio from the Cox proportional hazard model for the Abilify Maintena to placebo comparison was 0.451 (95% CI = 0.299, 0.678), subjects in the Abilify Maintena group had less than half the risk of experiencing recurrence of any mood episode compared with subjects in the placebo group. Thus, superiority of Abilify Maintena over placebo was established. The analysis of the primary efficacy endpoint is shown in the Kaplan-Meier curves as follows (Figure 4). (See Figure 4.)
Click on icon to see table/diagram/image
Secondary and other efficacy endpoints were generally supportive of the primary efficacy outcome.
Abilify Maintena as maintenance treatment in adults with bipolar I disorder was assessed in a 52-week multicentre, open-label trial (n=464, Trial 31-08-252). Safety and tolerability were supportive of the results observed in the double-blind, placebo-controlled study.
Pharmacokinetics: Absorption: Aripiprazole absorption into the systemic circulation is slow and prolonged following Abilify Maintena administration due to low solubility of aripiprazole particles.
The average absorption half-life of Abilify Maintena is 28 days. Absorption of aripiprazole from the IM depot formulation was complete relative to the IM standard (immediate-release) formulation. The dose adjusted C
max values for the depot formulation were approximately 5% of C
max from IM standard formulation.
Following a single dose administration of Abilify Maintena in the deltoid and gluteal muscle, the extent of absorption (AUC) was similar for both injection sites, but the rate of absorption (C
max) was higher following administration to the deltoid muscle.
Following multiple intramuscular doses, the plasma concentrations of aripiprazole gradually rise to a maximum plasma concentration at a median t
max of 7 days for the gluteal muscle and 3 days for the deltoid muscle.
Steady state concentrations for the typical subject were attained by the fourth dose for both sites of administration.
Less than dose-proportional increases in aripiprazole and dehydro-aripiprazole concentrations and AUC parameters are observed after monthly Abilify Maintena injections of 300 mg to 400 mg.
Distribution: Based on results from trials with oral administration of aripiprazole, aripiprazole is widely distributed throughout the body with an apparent volume of distribution of 4.9 l/kg, indicating extensive extravascular distribution. At therapeutic concentrations, aripiprazole and dehydro-aripiprazole are greater than 99 % bound to serum proteins, binding primarily to albumin.
Biotransformation: Aripiprazole is extensively metabolised by the liver primarily by three biotransformation pathways: dehydrogenation, hydroxylation, and N-dealkylation. Based on
in-vitro studies, CYP3A4 and CYP2D6 enzymes are responsible for dehydrogenation and hydroxylation of aripiprazole, and N-dealkylation is catalysed by CYP3A4. Aripiprazole is the predominant medicinal product moiety in systemic circulation. After multiple dose administration of Abilify Maintena, dehydro-aripiprazole, the active metabolite, represents about 29.1-32.5 % of aripiprazole AUC in plasma.
Elimination: After administration of multiple dose of 400 mg or 300 mg of Abilify Maintena, the mean aripiprazole terminal elimination half-life is respectively 46.5 and 29.9 days presumably due to absorption rate-limited kinetics. Following a single oral dose of [
14C]-labelled aripiprazole, approximately 27 % of the administered radioactivity was recovered in the urine and approximately 60 % in the faeces. Less than 1 % of unchanged aripiprazole was excreted in the urine and approximately 18 % was recovered unchanged in the faeces.
Pharmacokinetics in special patient groups: CYP2D6 poor metabolisers: Based on population pharmacokinetic evaluation of Abilify Maintena, the total body clearance of aripiprazole was 3.71 L/h in extensive metabolisers of CYP2D6 and approximately 1.88 L/h (approximately 50 % lower) in poor metabolisers of CYP2D6 (for dose recommendation, see Dosage & Administration).
Elderly: After oral administration of aripiprazole, there are no differences in the pharmacokinetics of aripiprazole between healthy elderly and younger adult subjects. Similarly, there was no detectable effect of age in a population pharmacokinetic analysis of Abilify Maintena in schizophrenia patients.
Gender: After oral administration of aripiprazole, there are no differences in the pharmacokinetics of aripiprazole between healthy male and female subjects. Similarly, there was no clinically relevant effect of gender in a population pharmacokinetic analysis of Abilify Maintena in clinical trials in patients with schizophrenia.
Smoking: Population pharmacokinetic evaluation of oral aripiprazole has revealed no evidence of clinically relevant effects from smoking on the pharmacokinetics of aripiprazole.
Race: Population pharmacokinetic evaluation showed no evidence of race-related differences on the pharmacokinetics of aripiprazole.
Renal impairment: In a single-dose study with oral administration of aripiprazole, the pharmacokinetic characteristics of aripiprazole and dehydro-aripiprazole were found to be similar in patients with severe renal disease compared to that in young healthy subjects.
Hepatic impairment: A single-dose study with oral administration of aripiprazole to subjects with varying degrees of liver cirrhosis (Child-Pugh Classes A, B, and C) did not reveal a significant effect of hepatic impairment on the pharmacokinetics of aripiprazole and dehydro-aripiprazole, but the study included only 3 patients with Class C liver cirrhosis, which is insufficient to draw conclusions on their metabolic capacity.
Toxicology: Preclinical safety data: The toxicological profile for aripiprazole administered to experimental animals by intramuscular injection is generally similar to that seen following oral administration at comparable plasma levels. With intramuscular injection, however an inflammatory response was seen at the injection site, and consisted of granulomatous inflammation, foci (deposited drug), cellular infiltrates, oedema (swelling) and, in monkeys, fibrosis. These effects gradually resolved with discontinuation of dosing.
Non-clinical safety data for orally administered aripiprazole revealed no special hazard for humans based on conventional studies of safety pharmacology, repeat-dose toxicity, genotoxicity, and carcinogenic potential.
Oral aripiprazole: For oral aripiprazole, toxicologically significant effects were observed only at doses or exposures that were sufficiently in excess of the maximum human dose or exposure, indicating that these effects were limited or of no relevance to clinical use. These included: dose-dependent adrenocortical toxicity in rats after 104 weeks of oral administration at approximately 3 to 10 times the mean steady-state AUC at the maximum recommended human dose and increased adrenocortical carcinomas and combined adrenocortical adenomas/carcinomas in female rats at approximately 10 times the mean steady-state AUC at the maximum recommended human dose. The highest non-tumorigenic exposure in female rats was approximately 7 times the human exposure at the recommended dose.
An additional finding was cholelithiasis as a consequence of precipitation of sulphate conjugates of hydroxy-metabolites of aripiprazole in the bile of monkeys after repeated oral dosing at 25 to 125 mg/kg/day or approximately 16 to 81 times the maximum recommended human dose based on mg/m
2.
However, the concentrations of the sulphate conjugates of hydroxy-aripiprazole in human bile at the highest dose proposed, 30 mg per day, were no more than 6 % of the bile concentrations found in the monkeys in the 39-week study and are well below (6 %) their limits of
in vitro solubility.
In repeat dose studies in juvenile rats and dogs, the toxicity profile of aripiprazole was comparable to that observed in adult animals, and there was no evidence of neurotoxicity or adverse events on development.
Based on results of a full range of standard genotoxicity tests, aripiprazole was considered non-genotoxic. Aripiprazole did not impair fertility in reproductive toxicity studies.
Developmental toxicity, including dose-dependent delayed foetal ossification and possible teratogenic effects, were observed in rats at doses resulting in sub-therapeutic exposures (based on AUC) and in rabbits at doses resulting in exposures approximately 3 and 11 times the mean steady-state AUC at the maximum recommended clinical dose. Maternal toxicity occurred at doses similar to those eliciting developmental toxicity.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image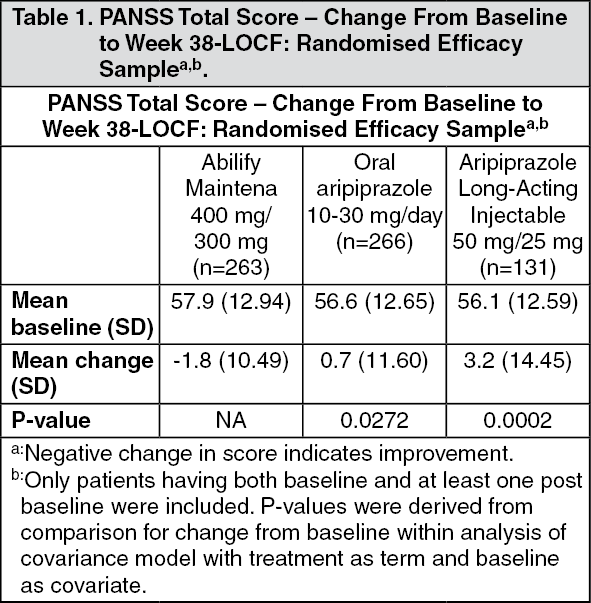 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image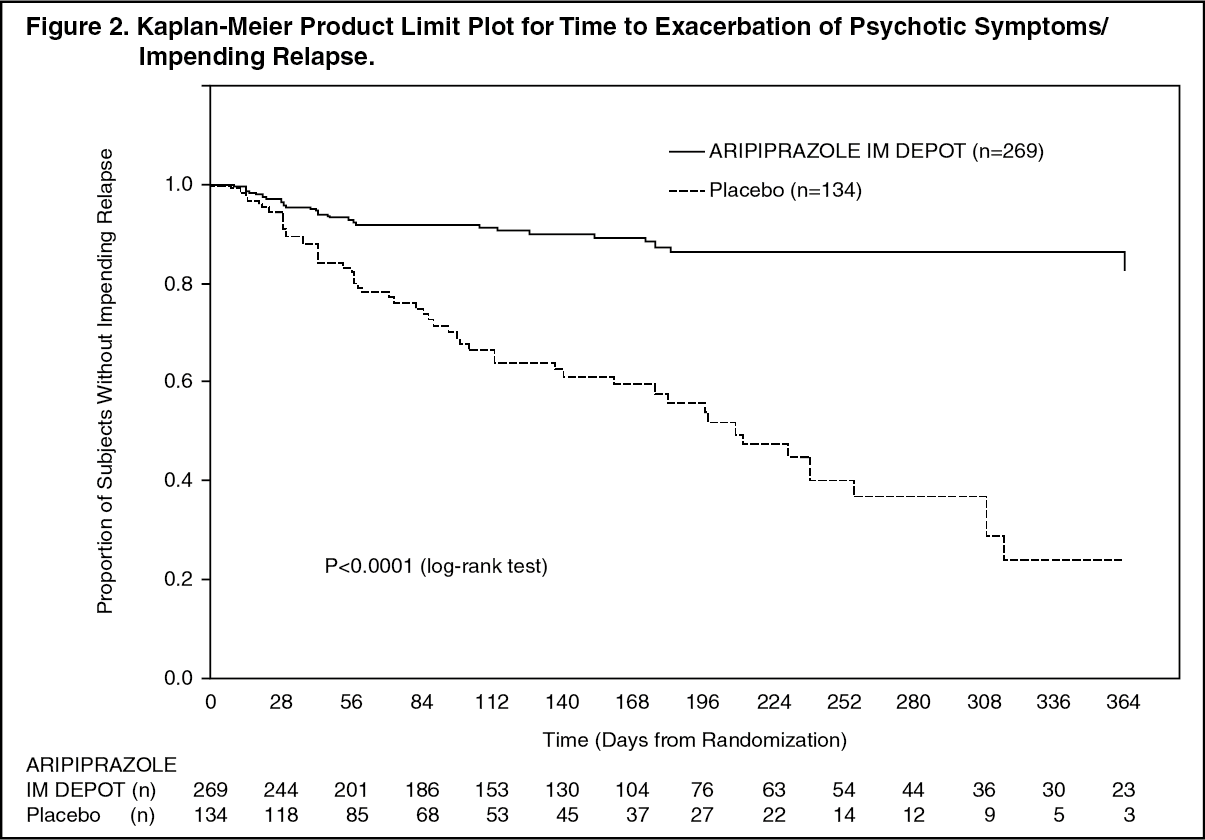 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image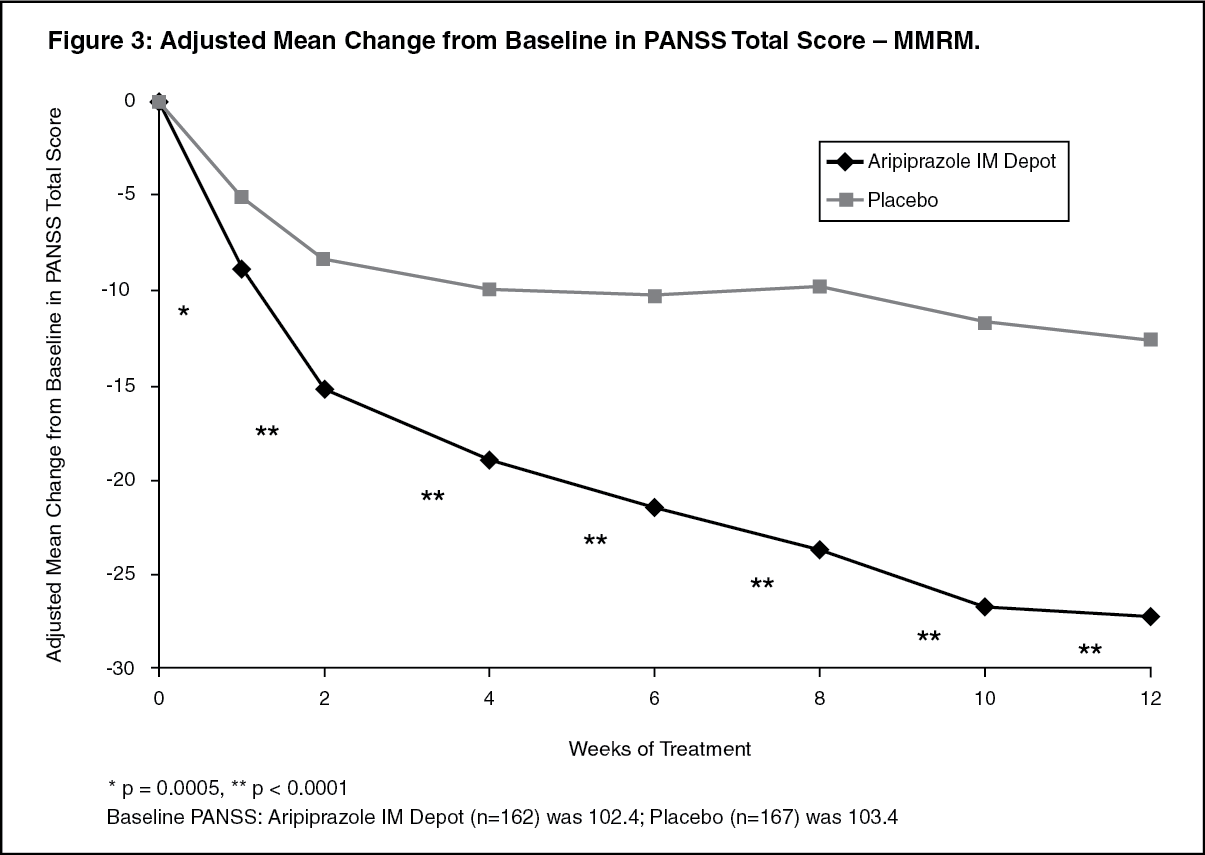 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image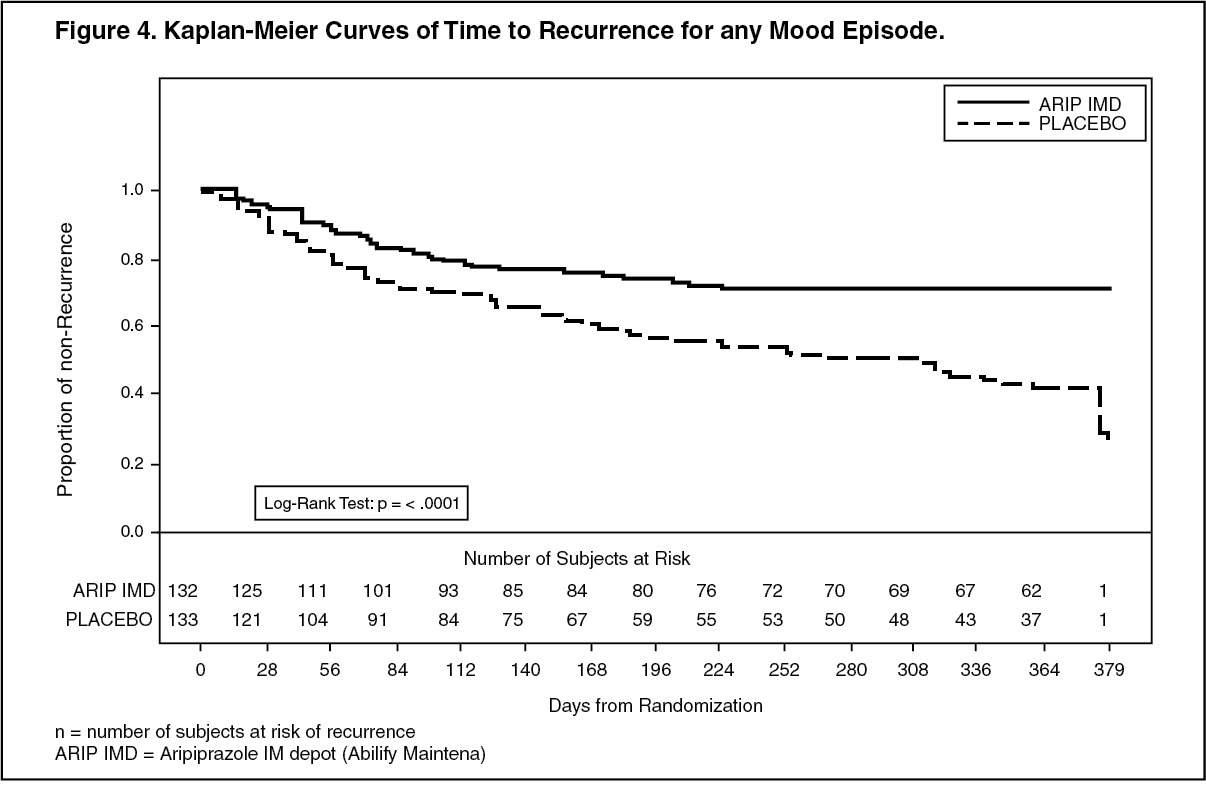 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image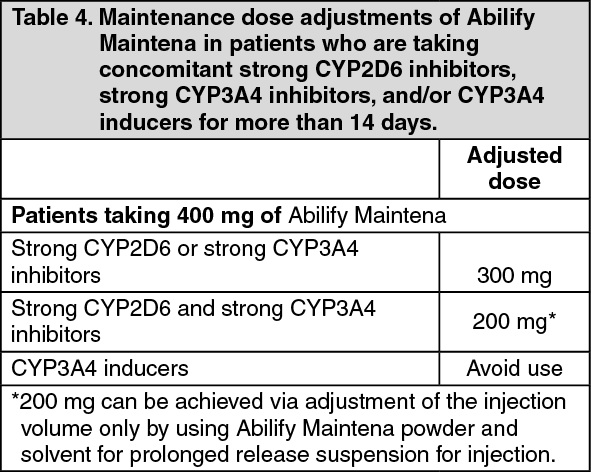 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image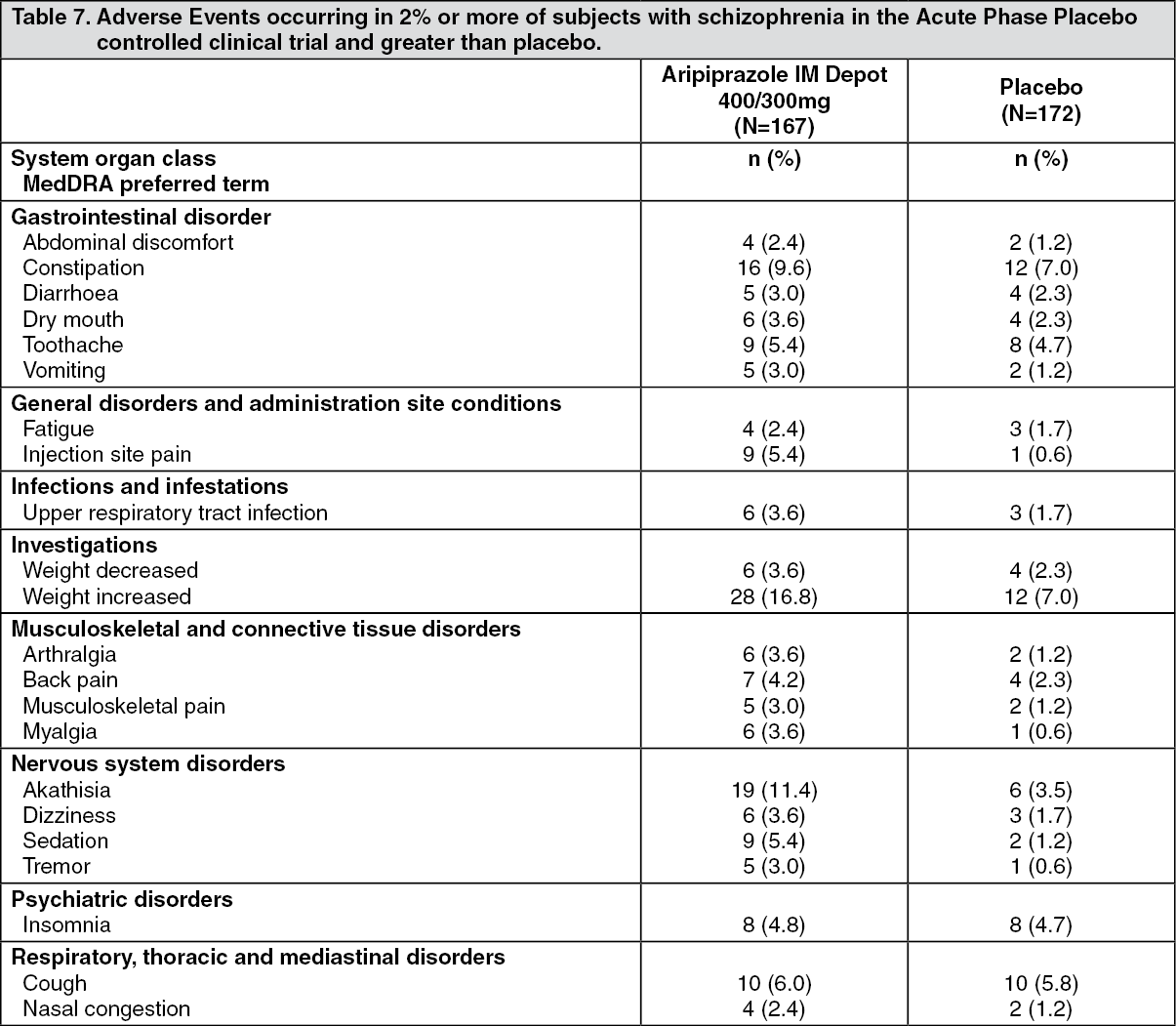 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image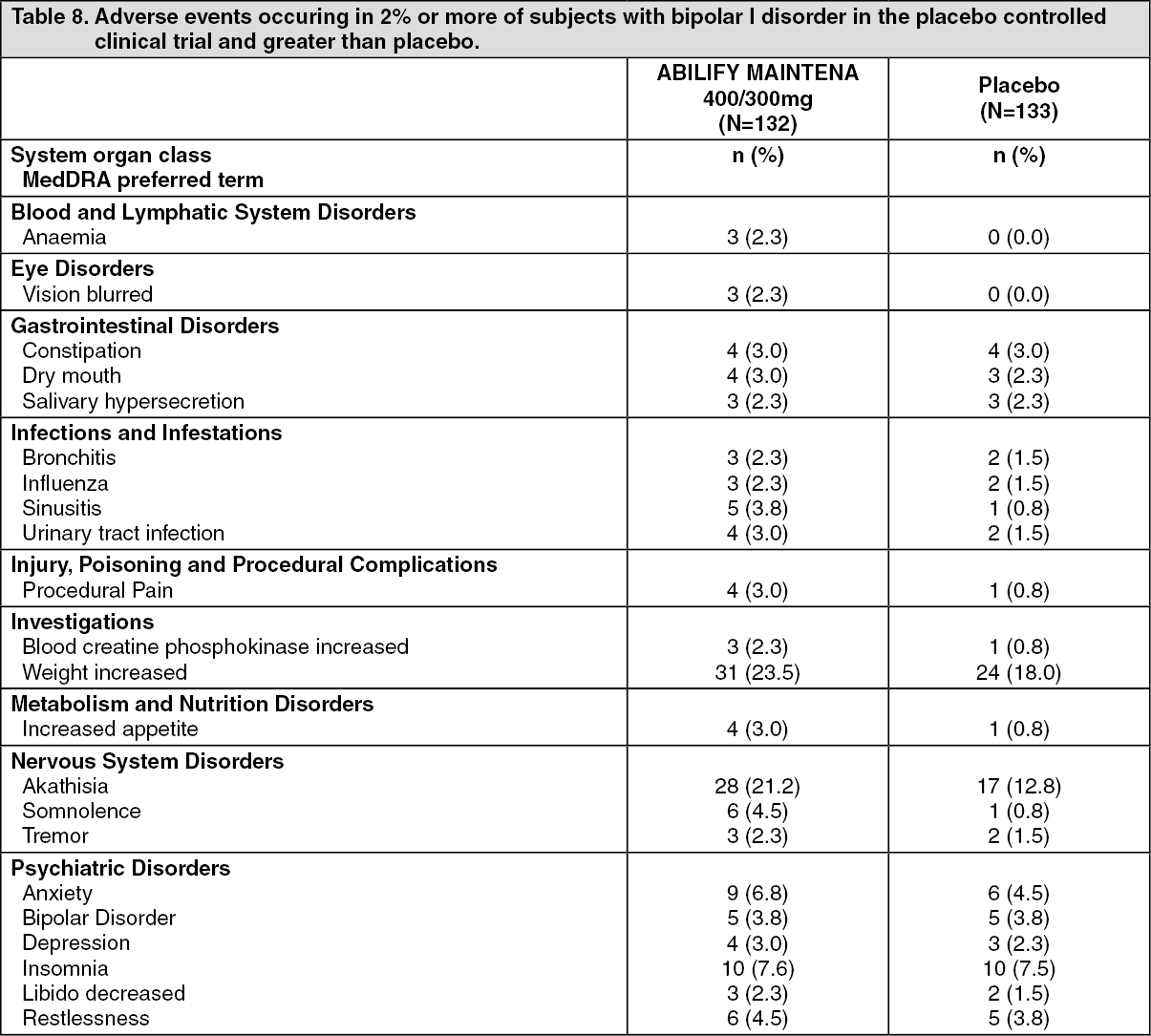 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image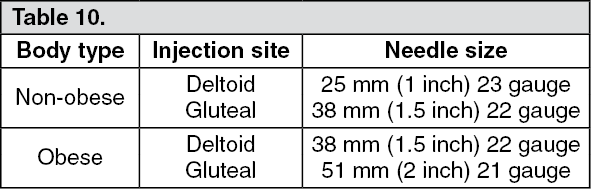 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image 400 mg8ac4bc07-0f11-4149-8cb9-a9d200980e10.GIF)

 Sign Out
Sign Out
